PET Basic 3
PET Basic 3
Uploaded on October 15th, 2020
By Dr. Riffat Parveen Hussain.
Consultant Nuclear Medicine Physician.
Department of Radiology.
Section of PET CT.
Jinnah Postgraduate Medical Centre.
Karachi
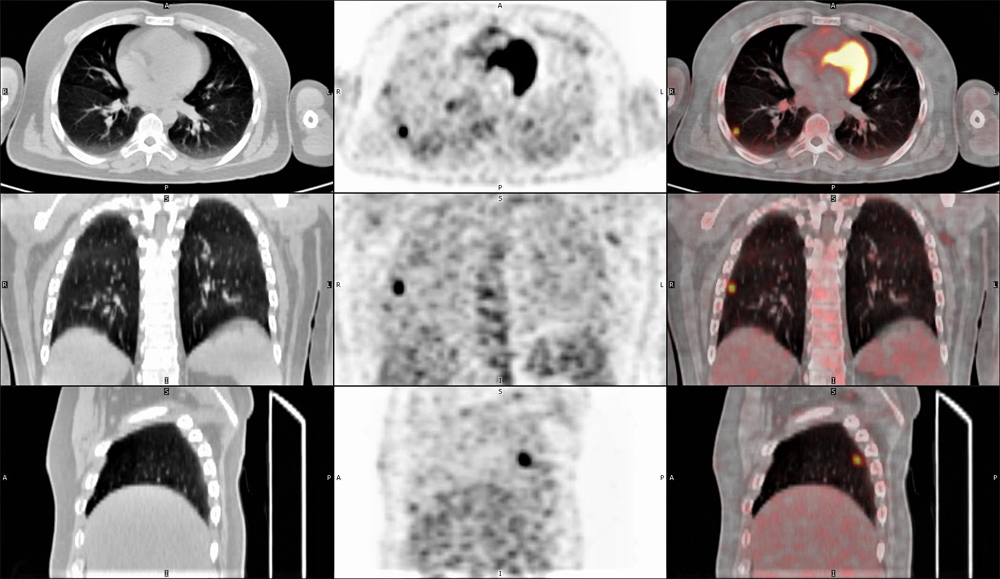
27-year-old male, known case of osteogenic sarcoma of left femur was sent for disease evaluation. He fasted for pay id casino 4 hours and had a blood glucose of 78 mg/dl; scan was done after 60 minutes of delay from the time of injection. In addition to the primary area of disease, a focal area of increased metabolic activity was seen in the lateral segment of the lower lobe of the right lung (figure1).
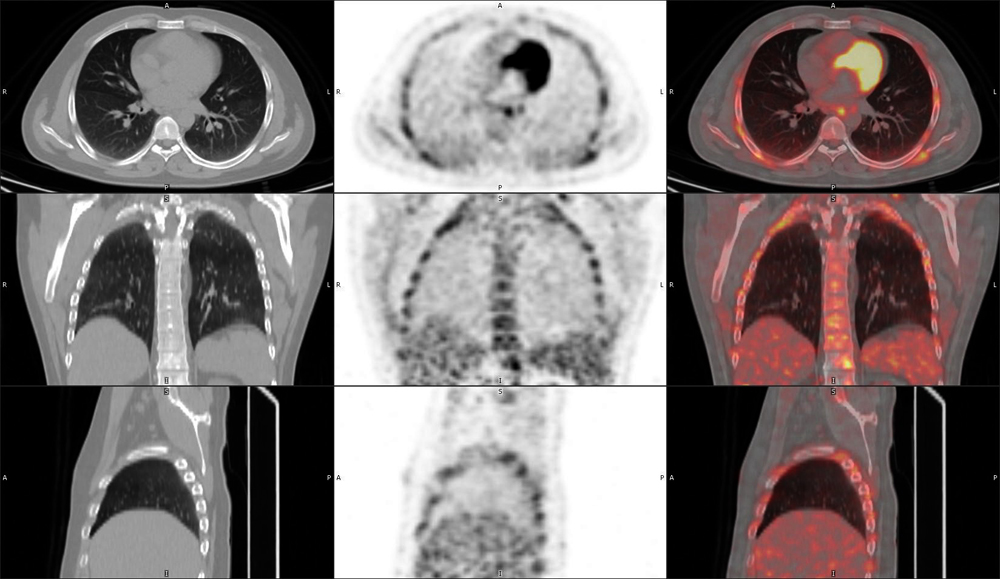
The patient was recalled after 4 days and the thorax was rescanned.
The follow-up scan showed no visualization of the previously noted uptake in the right lobe (figure 2).
What is the most likely cause/diagnosis: –
- Granuloma
- Hot clot artefact
- Metabolically active pulmonary nodule
- Primary lung mass
- Pulmonary metastasis
Scroll down for answer
Correct answer is option 2; Hot Clot artefact
Discussion
FDG uptake tracer in the lung can be the result of various causes which include, infection, inflammation, and primary pathology/metastases; all these are invariably associated with structural abnormality on CT (1,2).
There are instances, however, when focal tracer accumulation may be in evidence in the lung parenchyma without any evidence of any CT correlate. These uptakes are considered as “hot clot / emboli” artefact and may lead to false positive results if the corresponding CT image are not taken into consideration. The CT portion of the PET-CT is important to the scanning as it enables anatomical localization of lesions showing metabolic activity on PET scan (2–5).
A faulty technique of the injection of the radiotracer 18-FDG (aspiration of blood into the injector), has been cited as the cause for this “hot clot” / “emboli”.It is said to occur as a result of the agglutination of FDG by erythrocytes during the FDG injection. The resulting microemboli is then caught in the pulmonary vasculature which creates a focal FDG uptake on the PET images. As there is no associated morphological abnormality in the area of capture, the concomitant CT images reveal no associated pathology(2,4).
Though blood aspiration into the injector has been cited as the most common basis for the clot formation, paravenous injection and high speed injection may also be possible causes (4).
To make a diagnosis of hot-clot artifact there must be focal FDG uptake in the lung with no CT correlate. The SUV max of the lesion must be high and should disappear on repeat scanning with a proper injection technique (2,3), as was seen in this case.
Other causes for of focal metabolic area in the lungs on PET images without a CT counterpart have also been given with a mis-registration of PET and CT images being the most common.This is seen because of breathing movements and usually occurs at lung bases, diaphragm and upper abdomen; shallow breathing during chest acquisition is thus recommended to achieve optimal image fusion during PET-CT acquisition (2,6).
In addition to the above discussed causes, cases of iatrogenic embolism have also been reported in literature (7)
All answers, except for the correct one, should show associated morphological abnormalities on the CT images of the scan.
References
- Kumar K. Clinics in Oncology FDG Emboli on PET / CT Scan – A Case Report. 2016;1:1–2.
- Hussain R, Mahmood T. The hot embolus of 18 F-fluorodeoxyglucose. World J Nucl Med [Internet]. 2020;0(0):0. Available from: http://www.wjnm.org/preprintarticle.asp?id=290377;type=0
- Bikkina P, Kotha S, Ali Z. Abnormal Fluorodeoxyglucose Uptake in Lung without Structural Abnormality on Computed Tomography. Indian J Nucl Med [Internet]. 2017 [cited 2018 Oct 31];32(4):359–60. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29142360
- Ozdemir E, Poyraz NY, Keskin M, Kandemir Z, Turkolmez S. Hot-clot artifacts in the lung parenchyma on F-18 fluorodeoxyglucose positron emission tomography/CT due to faulty injection techniques: Two case reports. Korean J Radiol. 2014;15(4):530–3.
- Chondrogiannis S, Marzola MC, Grassetto G, Zorzi A, Milan E, Rampin L, et al. 18F-FDG PET/CT lung ‘focalities’ without coregistered CT findings: An interpretative clinical dilemma. Nucl Med Commun. 2015;36(4):334–9.
- Liu Y. Fluorodeoxyglucose uptake in absence of CT abnormality on PET-CT: What is it? World J Radiol. 2013;5(12):460.
- Hany TF, Heuberger J, von Schulthess GK. Iatrogenic FDG foci in the lungs: A pitfall of PET image interpretation. Eur Radiol. 2003;13(9):2122–7.