Cardiology Case 2
Cardiology Case 2
Uploaded on 1st May, 2020
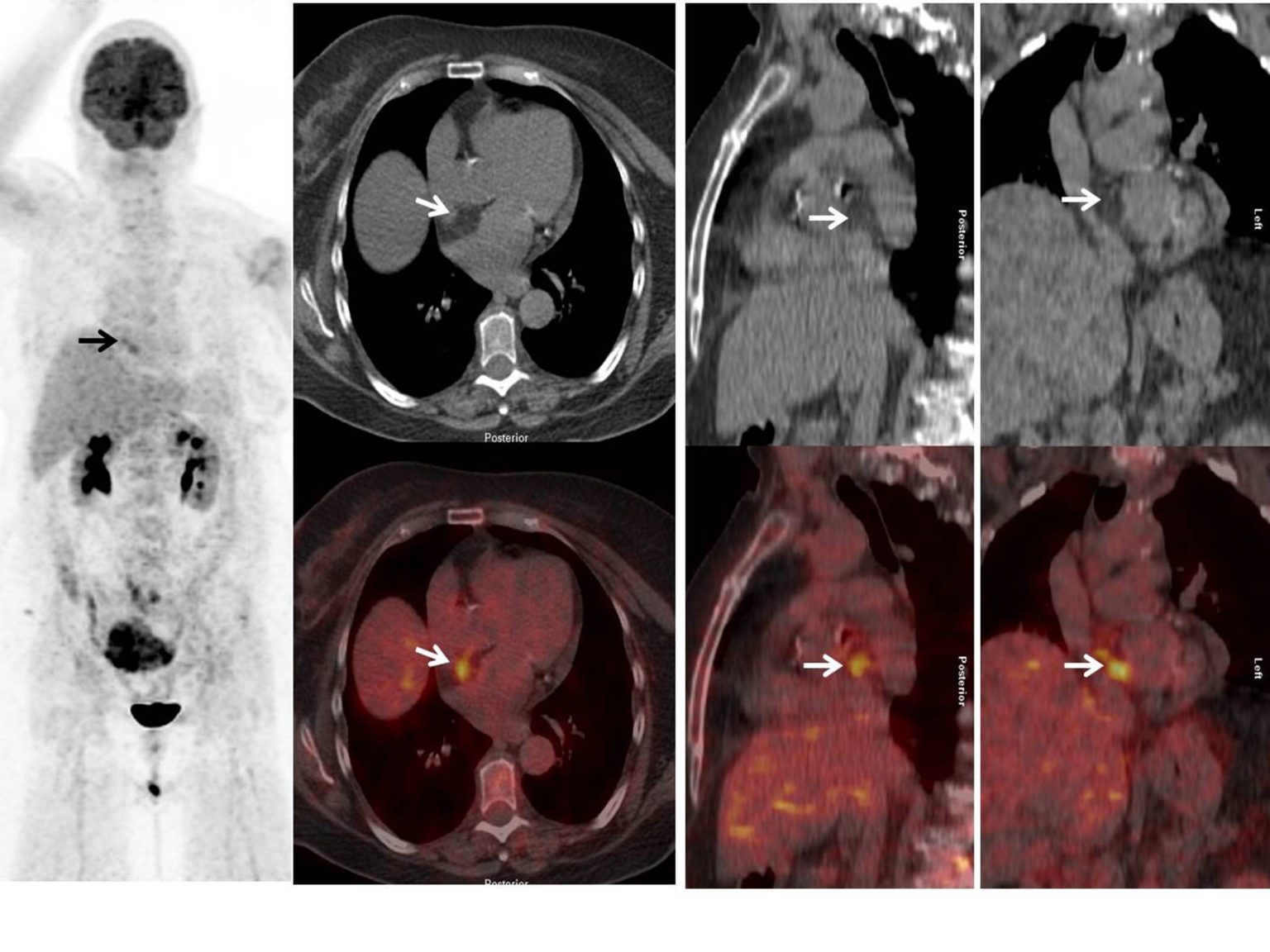
64-year old female is a known case of left breast cancer on follow-up. Recently presented with palpable left axillary lymph nodes and high tumor markers. 18F-FDG-PET/CT performed after injection of 5.2 mCi 18F-FDG for restaging. MIP 18F-FDG and cross-section 18F-FDG PET-CT images show focal increased tracer activity in the right side of the heart. What is the diagnosis ?
A. Focal FDG uptake in the right atrial appendage with no anatomic abnormality.
B. Focal FDG uptake in the interatrial septum corresponds with low attenuation on CT consistent with benign lipomatous hypertrophy.
C. Focal FDG uptake in the right atrial wall could be infective; for clinical correlation.
D. Focal hypermetabolic activity corresponding to low attenuating mass could be cardiac metastasis. Advised echocardiography.
Scroll down for answer
Answer B: Focal FDG uptake in the interatrial septum corresponds with low attenuation on CT consistent with benign lipomatous hypertrophy.
18F-FDG-PET/CT show focal 18F-FDG activity in the right side of the heart. Non-contract CT images shows the fat density in the interatrial septum (fatty expansion of interatrial septum) that spares fossa ovalis with corresponding increase tracer uptake on fused images. Increased FDG activity at the interatrial septum, corresponds to fat density on CT is consistent lipomatous hypertrophy of the interatrial septum (LHIS). LHIS is a relatively uncommon cardiac finding characterized by excessive deposition of adipocytes with varying quantities of brown fat. Brown fat in LHIS may be hypermetabolic on 18F-FDG PET/CT.
Lipomatous hypertrophy of the interatrial septum (LHIS) is a relatively uncommon anomaly of the heart characterized by benign fatty infiltration of the interatrial septum that usually spares the fossa ovalis [[i]]. Benign tumors such as myxomas, lipomas, papillary fibroelastomas, angiomas, and fibromas represent about 75% of primary cardiac tumors [[ii]]. The prevalence of LHIS is estimated to be between 1% and 8% [[iii]]. LHIS has been shown to cause electrocardiography changes, atrial arrhythmias, recurrent pericardial effusions and rarely sudden cardiac death [[iv]].
The majority LHIS are clinically silent and detected incidentally during routine chest X-ray, echocardiography, surgery or autopsy [[v]]. LHIS has a characteristic bilobed appearance on cross-sectional imaging at the level of the fossa ovalis due to fat accumulation in the anterior and posterior septum, with sparing of the fossa ovalis. The diagnosis is confirmed by detection of non-enhancing fat density on CT or fat signal intensity on MRI. It is distinguished from true intracardiac lipomas by its lack of a discrete capsule and its composition of both mature adipocytes and brown fat [[vi]].
LHIS can show increased FDG uptake on PET. This finding may be related to the presence of brown fat, which can be present in LHIS and has been reported to show increased FDG uptake in the rat model. In retrospective study by Fan et al [[vii]], reported that patients with LHIS demonstrated increased FDG uptake on PET with SUVs ranging 1.8 to 13.4, and it was postulated that these results might be explained by higher concentrations of brown fat in hypermetabolic lesions. It is importance to differentiate LHIS from other types of cardiac uptake related to primary cardiac tumors, metastasis or adjacent hypermetabolic nodal disease. Reading physicians should be familiar with this benign finding to avoid false positive interpretations.
[i]. Prior JT. Lipomatous hypertrophy of cardiac interatrial septum: a lesion resembling hibemoma, lipoblastomatosis and infiltrating lipoma. Arch Pathol. 1964;78:11–5.
[ii]. Heyer C, Kagel T, Lemburg S, Bauer T, Nicolas V. Lipomatous hypertrophy of the interatrial septum. Chest. 2003;124:2068–73.
[iii]. Meaney JFM, Kazerooni EA, Jamadar DA, Korobkin M. CT appearance of lipomatous hypertrophy of the interatrial septum. AJR Am J Roentgenol 1997; 168:1081-1084.
[iv]. Heyer CM, Kagel T, Lemburg SP, Bauer TT, Nicolas V. Lipomatous hypertrophy of the interatrial septum: A prospective study of incidence, imaging findings, and clinical symptoms. Chest. 2003;124:2068-73.
[v]. Cannavale G, Francone M, Galea N, et al. Fatty images of the heart: Spectrum of normal and pathological findings by computed tomography and cardiac magnetic resonance imaging. Biomed Res Int. 2018; 5610347.
[vi]. Page DL. Lipomatous hypertrophy of the cardiac interatrial septum. Human Pathol. 1970; 1:151-163.
[vii]. Fan CM, Fischman AJ, Kwek BH, et al. Lipomatous hypertrophy of the interatrial septum: increased uptake on FDG PET. AJR Am J Roentgenol. 2005; 184:339–342.